Calming the Storm
By Quinn Eastman
 |
||||
|
Flipping the switch: Targeting depression's neural circuitry |
Calming the Storm: Reducing epileptic seizures |
Capping the overflow: Easing dystonia symptoms |
||

As her doctors told Paula Moreland how they were proposing to treat her seizures, her eyes grew wide. Moreland's mother, who was with her at the appointment, said, "Just listen to them, babe."
|
|
A surgeon would implant an electrical stimulation device deep within her brain. The device would deliver current to calm the storms of signals that would sometimes erupt and cause her to lose consciousness. Moreland had already seen several neurologists and tried a variety of anti-seizure drugs. At one point, she was taking seven different medications. "They didn't seem to work, and they made me sick," she says. "I went to talk with one doctor, and he threw up his hands. It was like he was saying, 'I give up.' "
Epilepsy seemed to have come into her life out of nowhere, Moreland recalls.
A divorced mom, she was traveling often for her job at a telecommunications company. Her doctors hypothesized that a car accident in Florida may have stirred up the seizures, but a precise cause was never pinned down.
Twice, seizures occurred while she was driving. She doesn't remember the accidents that followed, but she does remember the odd feeling (sometimes called an "aura") that preceded them. She once lost consciousness after a seizure at a bible study meeting.
Her family suggested that she see doctors at Emory, where she underwent diagnostic procedures, including surgery, that kept her in the hospital for a month and led to painful swelling. Her daughter started crying when she saw her with a shaved head. "I laugh about it now, but it was hurtful then," Moreland says.
Loss of control
Thomas Henry, the former head of Emory's epilepsy program, described deep brain stimulation to her. It may have seemed risky to try an experimental procedure, but Moreland was willing to take the risk. "If I had to choose between the epilepsy and having only one leg or one arm," she says, "I would not choose epilepsy, because of the loss of control."
At that point, the only tested-and-proven measure against drug-resistant epilepsy was surgery to remove the part of the brain where seizures originated. In Moreland's case, that region was the hippocampus: the same region she depended on for remembering words and forming memories.
"That's the reason why we thought she was a good candidate [for deep brain stimulation] and why she was enrolled," says neurosurgeon Robert Gross. "The only other option at that time was to resect the temporal lobe on her language-dominant side. If she experienced negative effects, we could simply shut the current off or even take the device out if it was completely ineffective."
Two wires were inserted under the skin of her head and carefully positioned through two small drill holes that lead to the region of the brain called the thalamus. The wires run down her neck and are connected to an electrical stimulator with a battery implanted under her collarbone. Now, several years after surgery, Moreland is nearly seizure-free. She continues to take the anti-seizure drug carbamazepine. She says there are some effects of the stimulation on her short-term memory. "I need to write things down," she says. "I can remember things from 20 years ago, but sometimes my family needs to remind me about something I did just a little while ago."
Moreland is an active community volunteer and writes, directs, and produces gospel plays. Still, it took seven years before she had the confidence to drive again, and she does not go long distances. She says she is blessed to have a large group of supportive friends and relatives. Her plays have been performed at community venues such as Big Miller Grove Baptist Church, where she is a member, and at her alma mater, Liberty University. She also appears as an extra in the film Selma. "I feel like a walking miracle," she says.
Daring treatment
|
|

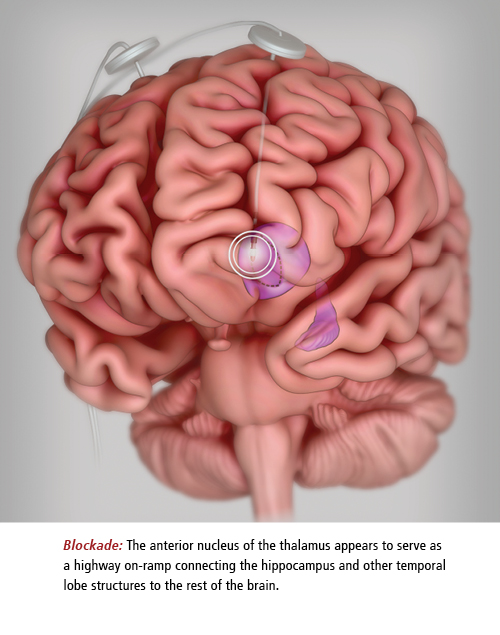
The basic idea underlying Moreland's treatment is this: if electric stimulation with the right frequency can restrain activity in a key bottleneck area, seizures won't spread. Many patients with drug-resistant epilepsy have seizures that begin in the temporal lobe. The anterior nucleus of the thalamus (or ANT) appears to serve as a highway on-ramp connecting the hippocampus and other temporal lobe structures to the rest of the brain.
These observations led to small studies of the effects of stimulating the ANT in patients with drug-resistant epilepsy as early as the 1960s. Subsequent success with deep brain stimulation in Parkinson's, along with experiments with animal models of epilepsy, led to further studies of ANT stimulation in epilepsy patients in the 1990s.
The first multi-center controlled trial, which Moreland participated in, didn't start until 2003. SANTE (Stimulation of the Anterior Nucleus of the Thalamus in Epilepsy) was sponsored by the medical device company Medtronic. Most of the 110 participants saw a reduction in the frequency of their seizures of at least 50%, but that effect built up gradually over two years. Only a few were seizure free for six months or more. About a quarter of participants reported noticing some memory impairment, like Moreland.
Even after generally encouraging results from SANTE and a narrow vote in favor from an advisory panel, the FDA did not approve Medtronic's application in 2010, citing concern over safety and side effects. The device is approved in Europe, Canada, and elsewhere. Medtronic has reapplied to the FDA, armed with more long-term data on SANTE participants.
In 2013, the FDA did approve another deep brain stimulation (DBS) device as a treatment for drug-resistant epilepsy. The Responsive Neurostimulation System, made by Neuropace, targets a different region of the brain: the actual site of onset of the seizures in the cortex, including, in half the patients, the hippocampus itself. It is programmed to sense an oncoming seizure and respond with a burst of electricity. Gross is not yet satisfied with the reduction in seizure frequency seen in published clinical trials of DBS. "This is not a cure; this is a first step," he says.
Exactly how electrical stimulation works is poorly understood. Researchers first thought that high-frequency stimulation simply shut down some circuits in the brain but now believe its effects are more complex. The gradual improvement seen in trials suggest that the brain's circuits are remodeling in response to the stimulation.
Gross sees opportunities to refine electrical stimulation as technology advances. Industry scientists have developed finer electrodes with more contacts, making it possible to "steer current where we want it to go." Better MRIs can allow more precise electrode placement. Newer DBS devices can record electrical signals from inside the brain over time. And a better understanding of how seizures spread in the brain could make it possible to design treatments for patients whose seizures originate outside the temporal lobe. "My concern is that the field will settle for something that is just good," Gross says. "The question now is, how do we make this therapy great?"
Related Resources:

