Caring For the Poor
By Mike King
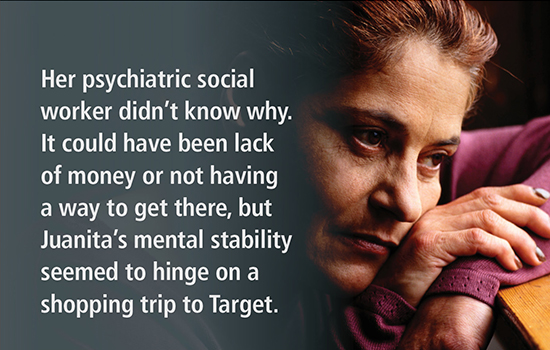
 "I think she needs some bras," a member of Grady Hospital's Assertive Community Treatment team tells her colleagues as they go through, one by one, a long list of names staring at them on the whiteboard. "It's made her increasingly anxious."
"I think she needs some bras," a member of Grady Hospital's Assertive Community Treatment team tells her colleagues as they go through, one by one, a long list of names staring at them on the whiteboard. "It's made her increasingly anxious."
"I'll get you some money," the team's leader said. Another team member jumps in, volunteering to take Juanita to Target the next day.
The next name on the team's board is Peggy, who has temporarily stopped taking her antipsychotic medications, a team member reports. Peggy presented herself at Grady Hospital's ER two days before with a urinary tract infection, and she claimed the ER nurses told her that her medications probably caused her infection.
"I had to sit down with her and go over her discharge papers to show her that's not what they were saying," the psychiatric nurse presenting the case tells the team. The next team member who sees her should follow up that she is taking both her psychiatric meds and the antibiotic she was prescribed for her infection.
Two down. The team has about 58 names to go — all patients with similar stories revealing precarious control over their illnesses.
To me, an outside observer who agreed as a condition of attending the meeting not to use the real names of clients, the team's ability to succeed with many of the patients seems equally precarious, especially given how fragmented and unresponsive the American health care system can be for the chronically mentally ill.
There are success stories, to be certain. The team cheers news of a new job for one of the patients, or a new, more stable living arrangement for another. Robert has reconciled with his brother, who says he'll give him another chance. Rose got her old job back. Jackie's estranged daughter has moved back to town, and she sees her once a week.
But even these patients are one unlucky break away from trouble. Something as random as an argument with a family member, a late Social Security check, an arrest for disorderly conduct, a frustrated municipal court judge who is tired of dealing with them can put them in jeopardy.
The team effort employed at Grady has been around for years. It was first successfully used in Wisconsin and based on a simple, but expensive premise: Chronic, severe mental illness requires more than short-term hospital stays, periodic outpatient group therapy, and daily medications.
It involves frequent, supportive contact that ensures patients don't get sidetracked by what most of us would consider minor setbacks, like needing to go shopping. Most importantly, patients must be willing to agree to frequent interventions in order to participate in the program.
Grady has three Assertive Community Treatment teams that meet every weekday. Combined, they have a patient load nearing two hundred—by far the largest of any program like it in Georgia. Funding for the program comes from a variety of sources such as state and local grants, mostly, but also from Medicaid, if the patients are eligible for coverage.
Unfortunately, many aren't. They could be, but Georgia won't allow it. So the program stays permanently underfunded, forcing Grady to absorb the cost.
Picking up the pieces
The goal for each team is to see patients at least three times a week. These encounters are designed to determine if the patients are taking the medications they need, keeping their appointments, having any luck at finding work, and living somewhere that doesn't exacerbate their serious mental conditions.
The Grady program is handling an ever-increasing load. When the state system for caring for the poor and uninsured mentally ill essentially collapses, as it did in Georgia over the last ten years, it predictably falls on public hospitals and nonprofit charities to pick up the pieces.
If there is one medical condition where American medicine and public health policy has failed the poor and uninsured most, it is in mental health care. Despite numerous scandals and journalistic investigations over the years, public officials have rarely put forth efforts to comprehensively deal with it. Think of the last time a political campaign — any political campaign at any level — had a platform promising to fix the obvious failures in mental health financing or services for the poor.
What little progress that has been made on the subject has been to destigmatize chronic depression, bipolar disorders, schizophrenia, addiction, substance abuse, and other conditions as something more than just bad behavior. But "main-streaming" those disorders has largely been limited to patients who voluntarily submit to treatment and are covered by insurance when they need it.
Underlining the point, in the 1980s and 1990s, as mental health advocates began to make headway in demanding insurance companies cover psychiatric conditions the same way they cover other health issues, there was a surge in for-profit and private psychiatric hospitals opening to accommodate the demand.
Usually covered treatment began with a hospital stay to reestablish a medication regimen, followed by outpatient visits for psychotherapy, counseling, and medication compliance. How long the hospital stay was and how long outpatient care lasted depended largely on what was allowed under the patient's benefit plan. This is still largely the model used today for insured patients who need help coping with their illness.
But for the poor and uninsured, it is a much different world.
"Behavioral health for the poor is one of our most serious challenges, not just from the standpoint of what works and what doesn't, but because the numbers are overwhelming, and our system for paying for it has been cobbled together in crisis."
Dr. Bruce Siegel, president and CEO of America's Essential Hospitals
Private psychiatric hospitals and some acute-care hospitals with psychiatric beds may accept uninsured patients, often only to stabilize them and discharge them to their own care. But for the most part, these patients become the responsibility of the state mental health system, regional public health districts, the local public hospital, and, increasingly, the local jail and criminal justice system.
"Behavioral health for the poor is one of our most serious challenges, not just from the standpoint of what works and what doesn't, but because the numbers are overwhelming, and our system for paying for it has been cobbled together in crisis," said Dr. Bruce Siegel, president and CEO of America's Essential Hospitals, which represents most of the nation's largest safety-net hospitals. "Many states have simply defaulted on public mental health services and expect our hospitals to take on the responsibility."
Moreover, the promise of the 2010 health care reform law to provide coverage for more of the poor and uninsured — either through expanding Medicaid or through private plans that denied them coverage in the past — has also failed to materialize for many of these patients.
About twenty states, including Georgia, have refused to expand Medicaid coverage to residents who make too little to afford private insurance and too much to qualify for Medicaid under current guidelines. That effectively shuts out most of the uninsured mentally ill from the benefits of the new law. And it shifts much of the burden of paying for the care they inevitably need from the state onto public hospitals who have to treat them on an emergency basis.
The American Mental Health Counselors Association estimates that about one million Americans in need of mental health and substance abuse treatment did not receive it in 2014 because their states refused to expand Medicaid to cover them; more than 230,000 of these low-income and vulnerable patients reside in Georgia.
Over the last fifty years, the states and federal government have attempted to shift the burden of public health funding from one to the other with neither seemingly willing to accept the responsibility for coordinating care for a vulnerable and difficult-to-treat segment of society.
And while there is no winner in this standoff between federal and state health officials, there is no question who is harmed the most. The losers can easily be found on the streets of major cities, in county jails, and in overcrowded public hospital psychiatric wards.
The dismal record spans more than a century of public-policy indifference, stingy funding, unintended consequences, and fundamental misunderstanding of the nature of mental illness itself.
High cost of services
Unlike other chronic health conditions—such as heart disease, kidney disease, or even cancer, where symptoms are easy to diagnose and surgical treatment and medications can mitigate the impact of malfunctioning organs—chronic, serious bipolar disorders and schizophrenia manifest themselves in behavioral patterns that often are not easy to detect and even harder to control.
Insurance companies around the country report that they are having difficulty complying with the requirement written into the 2010 ACA that they treat mental illness on a parity with any other chronic medical condition they cover.
They complain that how to best diagnose and treat mental conditions is constantly evolving, making it difficult for insurers, especially HMOs, to provide adequate staff to meet what has turned out to be an unanticipated demand among newly insured patients.
In California, considered the "pace car of parity" for coverage of mental illness, Kaiser Permanente, which insures 7.5 million members in the state, was fined for not providing timely care to mentally ill patients. Its defense was that it did not have the staff and the paperwork requirements in place to monitor compliance with the law. (It does now, the company said.)
While there is no surgical procedure to deal with severe mental illness, fortunately there are drugs to control it. But treatment involves strict compliance and a supportive environment for those afflicted with the most serious forms of these illnesses. For many individuals, especially the poor, the supportive environment simply doesn't exist and must be taken up by the public health system.
Grady CEO John Haupert said the cost of behavioral health services for hundreds of severely mentally ill patients is one of the biggest threats to the bottom line of the state's largest safety-net provider. The high cost of services Grady must provide — especially to those patients who return time and again for inpatient care because they can't take care of themselves — crowds out the hospital's ability to provide care for poor and uninsured patients with other conditions.
Even if Georgia had agreed to the Medicaid expansion, Grady would still have been hard-pressed to provide the volume and intensity of services these patients need, Haupert said, because direct state funding for mental health services has been reduced across the board.
Nationally, per capita public health spending on mental health services by the state was roughly $120 in 2013. Georgia spent less than half of that, according to data compiled by the Kaiser Family Foundation. It's little wonder then that state and local governments reimburse Grady for only about half of the cost of the services it provides for the uninsured mentally ill.
Boarding patients in the ER
More than 25 patients a day come to Grady's ER with psychiatric symptoms as their primary diagnosis. The hospital's inpatient behavioral health unit has almost tripled in size since 2012. It routinely has 80% occupancy and is often too full to take patients from the ER.
Public hospitals around the country report problems similar to Grady's, with other emergencies being crowded out of ERs because of the volume of mentally ill and substance abuse cases, Siegel said.
The American College of Emergency Physicians in 2014 reported that 84% of their members said they routinely have to "board" psychiatric patients in the ER—meaning the patients spend at least a day in the ER before a bed on a psychiatric ward became available.
 Many of those waiting patients — more than 90% of them, the ER physicians said — were considered so ill that caring for them in that setting distracted the staff and resulted in reduced services to other ER patients.
Many of those waiting patients — more than 90% of them, the ER physicians said — were considered so ill that caring for them in that setting distracted the staff and resulted in reduced services to other ER patients.
Moreover, there is a shortage of beds set aside specifically for emergency psychiatric care in many urban areas. Patients who get admitted may not be able to stay as long as they need to get stabilized and provided with an outpatient treatment plan.
This crisis in deciding who is responsible for treatment and social services for the chronically mentally ill is but the latest iteration in what can best be described as the country's most serious failure in ensuring health care for the poor.




